When Murphy Munday went into labor in 2017 a month early and took a Lyft to the hospital, she prayed she wouldn’t give birth to her first child in the back seat of a stranger’s car. Just 10 minutes after hurtling through the hospital doors, her daughter, Elliot, was born healthy and required no treatment beyond what a standard, full-term delivery would dictate. Munday, a 36-year-old fine artist from New York, had an uncomplicated, unmedicated vaginal delivery; she stayed in the hospital for two nights before returning home with her husband to start their new life as a family of three. A month later, the bills started to arrive, totaling more than $100,000.
The astronomical amount was partly due to the fact that the hospital needed to fully staff up, including neonatal intensive care nurses and C-section prep in preparation for a premature delivery. But for most women, health insurance would have helped cover the lion’s share of that. Munday had insurance, but it didn’t cover pregnancy or related costs. She and her husband, both freelancers, had an independent, high-deductible, self-pay plan that cost $1,200 a month for the two of them. (She declined to name the company but said, “It’s one of the biggies.”) When she conceived at age 31, “I never even thought being pregnant would not be covered,” so she didn’t call to confirm. Then the bills for her routine prenatal care—checkups, ultrasounds, IV fluids when she ended up in urgent care dehydrated—began showing up. Munday called her insurance company “and they said I didn’t have coverage for anything pregnancy-related. They said it was ‘too late.’ If I had called before conception, they could have adjusted my premium.”
So here she was, a new mom with a four-week old infant, “on the phone with the hospitals, the insurance company, anyone who would listen, bawling about owing over $100,000 in medical debt.” The insurance company reassured her they would renegotiate her fees, but Elliot’s bills were not covered. Ultimately, the charges were reduced to $40,000 (half of that discount was from the insurance company’s negotiations and half was from a credit granted by the hospital’s finance department), “and we’ve been paying off $40,000 ever since—for a birth that went from ‘Did my water break?’ to delivery in under two hours,” she says. “Every month I need to log in and make a payment, and I get mad every single time. My emotions are mixed: I feel so stupid for not checking, but at the same time, I’m like, ‘Why should I have to check on this? It should be such a standard part of insurance.”
The price of health when you’re a woman
Munday’s insurance debacle is emblematic of a problem experienced by millions like her, pregnant or not, every day: the lack of coverage (and associated overcharging) for basic medical costs associated with being a woman.
Prior to the passing of the Affordable Care Act (more affectionately known as Obamacare) in 2010, a third of women who attempted to purchase a health plan on their own were either turned down, charged a higher premium because of a pre-existing condition, or had specific health problems excluded from their plans, says The Commonwealth Fund. Simply checking “female” on your health insurance form when buying insurance on the individual market could result in monthly premiums 10 to 80 percent higher than for men.
This practice, called “gender rating,” also occurred with employer-based insurance and collectively cost women a billion dollars a year, fueling what the National Women’s Law Center (NWLC) called “a hostile environment for women.” Insurance expert Sally Poblete, who once led product development at Anthem and is currently head of provider experience at Circulo Health, an insurance plan endeavoring to transform health insurance for the Medicaid population (most of whom are women and children), says gender rating stemmed from the fact that women have long been considered “riskier” than men because “we live longer, we deliver babies and men don’t, and therefore women have higher costs.”
Thanks to the Affordable Care Act (ACA), gender rating is no longer legal, nor is the practice of denying coverage or charging inflated premiums for pre-existing conditions, says Alina Salganicoff, PhD, Director of Women’s Health Policy at the Kaiser Family Foundation. This is true regardless of whether you get your insurance through the Marketplace or your employer. The ACA requires private insurance and Medicaid expansion plans to cover key recommended preventative services, such as well-woman visits, birth control, mammograms, and screenings for osteoporosis, cervical and colon cancer, and gestational diabetes, with no deductibles or copays.
Women live longer, we deliver babies and men don’t, and therefore women have higher costs.
The ACA also greatly improved maternity coverage, with routine prenatal care now covered for everyone, regardless of whether you have insurance through the Marketplace, an employer, or Medicaid. (Medicaid covers approximately 40 percent of all pregnancies in the United States.) But Rachel Bervell, MD, MS, a Boston-based obstetrician and co-founder of The Black OB-GYN Project, says that different plans have different definitions of “routine prenatal care”—one might consider genetic testing for certain chromosomal abnormalities routine, while another doesn’t—resulting in hefty copays and bills for new moms. (The average national cost of childbirth for someone with employer-sponsored insurance was $13,811 in 2020.)
In the case of $100,000 delivery bills like Munday’s, Bervell speculates that because the ACA didn’t officially outlaw gender rating until 2014, Munday’s insurance company and others like it were able to slide through some loopholes; it may be that her plan was “grandfathered in,” says Salganicoff, meaning it didn’t have to offer the same rights and protections provided under the ACA, including maternity care.
There is, of course, far more to being a woman than having babies and getting routine mammograms. When it comes to the medical realm of womanhood, we face a slew of unique challenges. Among them: Miscarriage, depression, endometriosis, debilitating period pain, infertility, menopause, and chronic health issues such as heart disease and Alzheimer’s disease (both of which strike women with fierce tenacity once we lose the health-protective effects of estrogen during menopause).
For all these reasons and others, women have long been more likely than men to be found sitting in the average doctor’s waiting room…and that image has been used as ammunition by insurance companies, who have historically treated womanhood as a pre-existing condition.
For women, the system is still broken
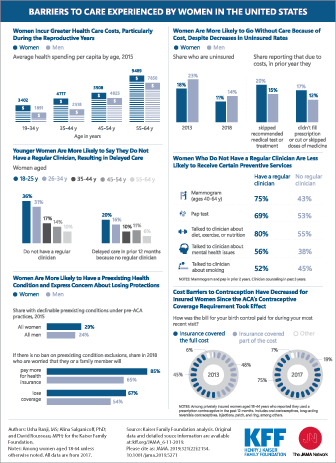
Despite improvements to Medicaid, the protection of the ACA, and the group purchasing power afforded by many employee-based insurance plans, women continue to shell out undue amounts of money for the most basic of health care necessities. In a 2021 Medicare Advantage survey of 1,017 women, roughly six in 10 said they believe they pay more for health care than men. They’re right: Across every age group, women are saddled with higher health care costs than men. According to data from a KFF-Journal of the American Medical Association collaboration, women aged 35-44 spent almost double on healthcare in 2019 compared to men.
For instance, while the ACA and most state Medicaid programs require coverage for preventive health care—an annual well-woman visit, for instance—without cost sharing (meaning deductibles, coinsurance, or copayments), nearly half of women report having to pay at least some out-of-pocket costs for these services, according to the 2020 Kaiser Family Foundation Women’s Health Survey. That includes 47 percent of women with private insurance plans, “most of which are prohibited from charging cost sharing for check-ups/well-woman visits and many preventive services,” the report says. This gap may be due to additional health services received during that visit, including diagnostic labs or tests, or as a result of patients needing to use out-of-network providers.
When it comes to treating miscarriages, infertility, and menopause, insurance coverage varies greatly. One in 10 women have experienced a miscarriage in their lifetime, according to a 2021 Lancet study, and recovery can cost thousands of dollars, depending on whether a woman needs a dilation and curettage (a surgical produce to remove the fetus, average U.S. cost of $7,296), anesthesia (to get her through that grueling procedure), and follow-up tests. One woman profiled by Slate.com reported that her miscarriage cost $17,000, and she ended up paying more than her $5,000 deductible. “I thought this would be covered under pre-natal care,” says another woman on an Elle.com video about the cost of miscarriages in the U.S. “That was the furthest thing from my mind, that insurance wouldn’t cover it.”
Bervell says that if you have a miscarriage and are on Medicaid, it is considered a delivery and the dilation and curettage would be covered. But if you have private insurance, “it may or may not be covered. And if you’re uninsured, the costs of managing a miscarriage can be absurd. What if you have complications? Or they might say, ‘It’s no longer a pregnancy; we don’t need to guarantee you the same benefits.’”
Meanwhile, for the one in 10 U.S. women who have sought assistance for infertility, the average cost of a single round of in vitro fertilization (IVF) is between $12,000 to $17,000, not including medication or genetic screening for embryo health, which typically costs tens of thousands more. Only 19 states mandate some level of insurance coverage for infertility (New York, for example, stipulates that “fully-insured” health care plans for employers with over 100 employees must provide coverage for three IVF cycles, whereas California requires only certain insurers to offer coverage for infertility diagnosis and treatment), but even then, that doesn’t mean having a baby will be affordable.
“About 80 percent of people who undergo IVF fertility treatments have hardly any or no coverage and pay out of pocket,” says Halle Tecco, founder of Natalist, which provides evidence-backed fertility and pregnancy essentials with a net-zero plastic footprint. The costs can be $50,000 or more, she says, and many walk away without a baby.
As for the more than 55 million U.S. women—nearly a third of us!—currently in menopause, with an additional two million joining the club every year, seeking coverage for common symptoms like brain fog, weight changes, sleep disruption, fatigue, anxiety or depression, joint and muscular pain, night sweats, hot flashes, skin and hair changes, vaginal dryness, and mood swings, can be spotty at best. “If you have new depression during menopause, it will be covered based on what your insurance plan deems necessary,” says Bervell. “Disparities occur, though, because some treatment modalities may not be recognized as necessary.” For instance, an insurer may approve the cost of Hormone Replacement Therapy to treat hot flashes, but not bioidentical hormones to treat vaginal dryness.
Health plans really need to think about how they are pleasing women.
With mental health care, “the problem is there is no basic standard of care for coverage,” says Pooja Lakshmin, MD, and clinical assistant professor of psychiatry at George Washington University School of Medicine and Health Sciences. For instance, “Mental health might be covered but there [will be] very few in-network psychiatrists or psychotherapists.” Even when they are in-network, she says, the waiting lists can be interminably long.
When Munday sought help with the psychological transition into parenthood—a turbulent process for many new moms—she learned that her plan offered mental health care but the covered providers were geographically inaccessible and did not offer tele-medicine, which until COVID-19, was rarely covered by insurance. Her first therapist charged $600 for an initial intake and $400 for subsequent sessions, all out of pocket. (The average cost for a single therapy session in the U.S. frequently falls between $100 and $200, and most do not accept health insurance.)
Expenses like these can lead to women forgoing medication or much-needed care. Nearly 30 percent of American women say they’ve skipped a medication or refill because the cost was too high. Thirty-eight percent of women missed out on preventive care during the pandemic.
This sort of neglect makes even less sense when you understand how strongly women dominate healthcare buying and usage in the U.S., making 80 percent of household health decisions and comprising 65 percent of the healthcare workforce. “Health plans really need to think about how they are pleasing women,” Tecco says, “not just for the consumer’s own personal health but also because women are the Chief Medical Officers of their home, literally managing the health of everyone in the household.”
New options on the horizon
We’re finally at a point where, at least on paper, being a woman can’t be used against us, insurance-wise. But on the whole, insurance still isn’t working for women. “We haven’t, as a country, put our fists down and said, ‘Health care is a human right.’”
Is the answer to build some sort of utopian one-stop-shop “Women’s Health Insurance” policy, where all the healths—mental, reproductive, preventative, holistic, dental—are covered for all women at 100 percent? While such a concept (think: the Oscar for women) sounds “delightful,” as Poblete puts it, it’s not likely.
Rebekah Etheredge, a licensed insurance producer and Medicare expert based in Southern California, says trying to curate a plan that addresses all of a woman’s needs across her lifespan would be cost-prohibitive for insurance companies. “Women are diverse and health care needs change throughout their lives, so trying to curate a coverage plan that’s the same for a teenager and an 85-year-old might be difficult,” she admits. “You might have a younger woman hoping to conceive a baby and she might put more focus on robust fertility coverage, while a woman recently diagnosed with breast cancer might be more concerned with a plan with coverage for cancer screenings and treatment.”
Still, it’s worth noting that United Healthcare, for example, generated $4.9 billion in profit during the first quarter of 2020 alone. (United Healthcare declined to comment whether such comprehensive coverage for women would be plausible from a cost perspective.) Diverse representation at the highest decision-making ranks could be part of the problem. Only 13 percent of healthcare CEOs are female, and of the dozen major health insurance companies, all are led by men except for Anthem and BlueCross, which recently appointed women CEOs in 2017 and 2020 respectively. You don’t have to look much further than their 2021 joint partnership with Reno Doula Project, to make doula services available at no cost to pregnant members, to realize the positive ripple effects when women govern our country’s largest healthcare companies.
When I think of 'health insurance for women,' my gut reaction is, 'We just need existing health insurance to work for women, not [something] new'.
Additionally, Tecco is hopeful that the rise of freelance workers and self-employment will create much-needed competition for the insurance Marketplace, meaning more consumer choice. “When I think of ‘health insurance for women,’ my gut reaction is, ‘We just need existing health insurance to work for women, not [something] new,” she says. “That comes from policy and shifts in existing health plans’ ability to attract certain customers. Health plans have to adapt to this new world. They need to be more attractive, not just to an HR person, but to the consumer.”
Even small changes, like improving access to tele-medicine; allowing 90-day supplies of medication; and offering affordable plans with lower deductibles “can really help women get the care they need, faster and on a more regular basis,” Etheredge says.
In the meantime, employers themselves can adopt upgraded strategies to fill in the gaps left by insurance companies. Natalist, for instance, offers its employees at least three days of paid miscarriage leave, which don’t count as sick days. Tecco recently posted on Instagram that she herself has utilized this benefit, and is “grateful…to work somewhere where my colleagues care enough to recognize the unique grief that comes with losing a pregnancy. If you lead a company, please consider adding a bereavement policy for miscarriage. And make it broad enough to cover any parent regardless if they are carrying the pregnancy or not.” Other examples include employers offering coverage for mental health care, pelvic floor physical therapy, or breast milk shipping when working, nursing moms are traveling.
Carrot Fertility, co-founded in 2016 by Tammy Sun, is one company trying to put some extra muscle behind the effort. Sun spent $35,000 of her savings to undergo egg freezing, initially assuming it would be a covered benefit like medical, dental, and vision, only to learn it most definitely was not. She created Carrot Fertility as an employer-sponsored benefit, meaning companies provide a certain dollar amount (ranging from $10,000 to $80,000 or more) for employees, loaded onto a debit-like card that can be used at the time of service for approved fertility services such as fertility preservation (egg, embryo, and sperm freezing), intrauterine insemination, IVF, and surrogacy. Carrot Fertility co-founder and VP of Business Development Juli Insinger says the company negotiates discounts at fertility clinics and adoption and surrogacy agencies on behalf of its members, lowering costs by an average of 15-20 percent.
View this post on Instagram
Other female-founded healthcare startups offering employer-sponsored benefits programs as an “add-on” to lackluster insurance policies include Stork Club, which offers family-related coverage for everything from IVF to newborn care and milk shipping, Ovia Health, which covers fertility and family building, children’s health, behavioral health, and more, and Arrow, a benefits platform which provides services for mental health, fertility, childbirth, lactation, parenting, return-to-work, and back-up childcare. Meanwhile Peppy Health is an employer-paid for health app that specifically targets female employees who need support with menopause.
Such benefits improve employee loyalty, making employees feel more emotionally supported, and even enhance mental health. Specifically, research shows that depression levels in patients with infertility are comparable to people who have been diagnosed with cancer, Insinger says, adding that a “fertility benefits program is an investment in the mental health of employees who are struggling with fertility issues; it can have a significant impact on [their] well-being.”
Insinger wants employees to know that oftentimes, employee requests will motivate an employer to offer benefits. “Know your negotiating power,” she says. “Ask your HR leader whether the company offers extra benefits and, if so, whether there are any restrictions to care.” Carrot Fertility provides a form on its website where employees can request Carrot reach out to their company to let them know an employee is interested in having the benefit at work (anonymously or not). “Companies that offer fertility benefits that cover all paths to parenthood equally send a message to their employees that your organization supports all definitions of ‘family,’” she adds.
Inadequate health insurance reinforces arbitrary cultural norms
Backing up several steps, “the first order of business is making sure we have a system that can provide access to coverage for all women,” says Salganicoff, the Director of Women’s Health Policy at the Kaiser Family Foundation. Case in point: Having affordable health insurance tied to full-time employment is an imperfect system that left more than 2.3 million women without health insurance after losing their jobs between February 2020 and February 2021 due to COVID-19. “We have a real patchwork system, and a lot of women fall through the cracks, with low-income women disproportionately affected.”
Take the fact that pregnant women with incomes up to 138 percent of the federal poverty level (currently $21,960 annually for a family of three), are given Medicaid coverage that starts in the prenatal period and extends to 60 days postpartum, leaving many women without a pathway to coverage just two months after giving birth. This opens them up to serious, possibly life-threatening deficits in care, considering that nearly a quarter of pregnancy-related deaths occur 43 to 365 days postpartum. (Black and indigenous women are two to three times more likely to die from pregnancy-related causes, Bervell points out.) Even many student health plans provided by colleges and universities do not offer comprehensive maternity coverage, according to Young Invincibles, an organization focused on policy needs for younger Americans.
Such examples of inadequate insurance coverage serve only to reinforce already ingrained arbitrary cultural norms—that women only need 60 days of healthcare postpartum, or 12 weeks of postpartum leave. When the Family and Medical Leave Act was passed in 1993, it was originally proposed as six months of paid postpartum leave, but “it got whittled away to 12 unpaid weeks,” says Lauren Smith Brody, founder of The Fifth Trimester, a consulting firm that helps businesses support and retain parents by prioritizing women’s physical and mental health. “We have totally internalized this idea that 12 weeks is enough time,” she explains, “but science shows that most women need six months to heal from delivery, to feel ‘normal’ again, and to feel emotionally adjusted.”
Recently, there has been growing interest from federal and state policymakers, clinicians, and health advocates in expanding Medicaid’s postpartum coverage from 60 days to one year, and in April, Illinois became the first state to expand Medicaid coverage to one year postpartum, thanks to the American Rescue Plan Act of 2021, which affords states a new option to extend Medicaid postpartum coverage to 12 months. In the meantime, Brody encourages employers to offer—and therefore begin to normalize the nationwide need for—six months of paid parental leave, or extra back-to-work support and on-ramping through the six-month mark, as well as fertility care, miscarriage leave, and mental health care. Ultimately, though, says Sally Poblete, we need a health coverage system that is grounded in the unique needs of women as opposed to the general population. “We need insurance coverage that is more attentive and intentional about designing for [women’s] needs—coverage that won’t leave women like Munday saying things like, ‘I should have just delivered in the Lyft.’”
Leslie Goldman, MPH, is a women’s health writer for Prevention, Women’s Health, Better Homes & Gardens, Parents, TheGirlfriend.com and more. She is the author or co-author of several books, including Locker Room Diaries: The Naked Truth About Women, Body Image, and Re-imagining the “Perfect” Body and Brave Girls: Raising Young Women with Passion and Purpose to Become Powerful Leaders.



{kind=link}